



Whenever a patient injures their low back, a common thought is that a “disc has slipped”. It’s entirely possible that our patients are correct in their diagnosis – although the term ‘slipped disc’ is a bit of a misnomer. The reality of disc herniation is a little more complex than simply ‘slipping’.
Anatomy
First off, let’s discuss the anatomy of our spinal ‘discs’.
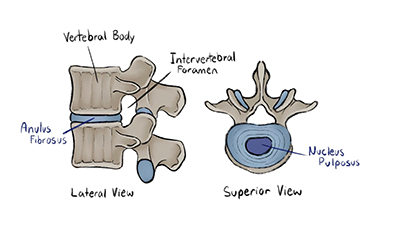
Our spines are made up of 24 vertebrae, each stacked on top of the other, separated by “intervertebral discs”. The discs themselves are comparable to that of a “Jelly Donut” you could grab from your local coffee shop. That is to say, they are composed of 2 layers – an outer, fibrous layer referred to as the Anulus Fibrosus (this would be the pastry component of the donut) & an inner, jelly-like layer referred to as the Nucleus Pulposus.
A true ‘slipped disc’, or disc herniation, occurs when the inner Nucleus Pulposus extrudes out from within the outer Anulus Fibrosus. In keeping with our Jelly-Donut metaphor, have you ever bitten into a Jelly donut, only to have the filling spill/burst out the side? That’s a disc herniation! As well, apologies if we’ve gone and put you off of donuts with this comparison.
Disc Herniation Stages
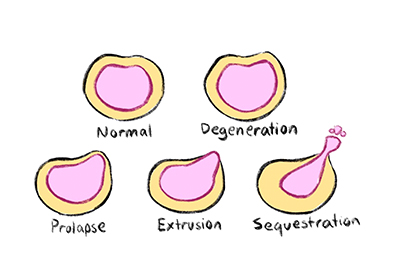
The above comparison describes an end-stage herniation, or sequestration. Disc herniations occur in stages or progressions, degeneration -> Prolapse -> Extrusion -> Sequestration. Symptoms may begin as early as the degeneration stage, although are more commonly found from prolapse onward. Extrusion describes the act of the Nucleus Pulposus ‘extruding’ out of the Annulus Fibrosus layer, and sequestration implies that the nucleus pulposus has completely exited the disc, and is free-floating within the spinal canal.
Disc Herniation Symptoms & Diagnosis
Perhaps counter-intuitively, the stages & progression of a disc herniation does not dictate the type of symptoms experienced (although there is possibly a correlation with the severity of those symptoms). Instead, the expected symptoms will vary based on the location of the disc herniation relevant to the surrounding structures.
Discs typically herniate in one of 4 possible areas, and each would make itself obvious based off of the group of symptoms the patient is experiencing. As well, the most common ‘levels’ of disc herniation are at L4-L5, & L5-S1 – either at the very bottom of your spine, or just above that.
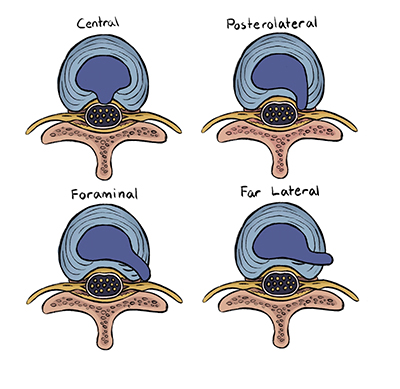
Central
This location occurs when the Nucleus Pulposus herniates straight back into the spinal cord. Patients with a central herniation will experience numbness and pain down the back of both legs, into the feet and may also lose bowel/bladder control. This is to be considered a medical emergency – patients should head to an ER immediately for surgical intervention or risk paralysis.
Posterolateral/Sub-articular
Just to the right-or-left of a central herniation, subarticular herniations do not impinge directly onto the spinal cord, but rather the small, ‘ventral’ (“from-the-front”) nerve fibers coming directly off of the spinal cord. Patients with sub-articular herniations may not experience numbness, but are more likely to have muscle weakness at the affected level. Patients with a subarticular herniation at the L4-L5 levels will have their L5 ventral nerve root affected – this would be tested for by having the patient walk ‘on their heels’ on the affected side. If the subarticular herniation is located at the L5-S1 level, the S1 ventral nerve root would instead be affected – patients wouldn’t be able to walk on their toes on the affected side.
Foraminal
All nerves in our body exit from our spinal canal and travel throughout our body. The passageways from which these nerves exit our spine are referred to as the “intervertebral foramen”. As such, a Foraminal herniation impinges right within that small exit-passageway. Patients would experience the same motor weakness as in sub-articular herniations, with the numbness/pain of central herniations occurring on the affected side only. These are perhaps considered the ‘classic’ disc herniation.
Far Lateral/Extra-foraminal
These herniations hurt. Outside of our spinal canals & just next to our vertebrae exist our “Dorsal-root Ganglia” – groups of Nerve cells who’s literal function is to transmit sensory information – including pain – to our brains. Extra-foraminal herniations may push right into these ganglia, and therefore patients will report much higher severity of perceived pain, yet have much better muscle strength over other herniation locations.
Treatment
Both conservative and surgical solutions exist for resolution of disc herniations. With the exception of central disc herniations, an argument could be made for beginning patients with a conservative, non-invasive course of treatment prior to surgery.
The goal of conservative treatment is to return the Nucleus Pulposus to the confinement within the Annulus Fibrosus through the use of negative pressure (movement is essential to this). Our discs are closed systems, or vacuums. In this line of thought – being able to ‘gap’ the space between our vertebrae results in the Nucleus Pulposus being more readily resorbed into its proper location. With conservative care, the average patient could expect to see 50% improvement within 6 weeks, with 90% of patients having full resolution of symptoms after 3 months.
A conservative treatment plan consists of chiropractic manipulation, mobilization & Extension-based (leaning backward) exercises in the ”McKenzie Protocol”. Massage Therapy would assist with pain relief during acute flare-ups, and continued chiropractic or physiotherapy care help to prevent recurrence once symptoms have abated.
Conclusions
Disc Herniations aren’t the most common cause of back pain, but are one of the more common concerns of patients. Depending on the progression and location of the herniation, patients may experience symptoms ranging from intense pain, to mild weakness, or nothing at all. Bowel or bladder dysfunction – that is loss of control or difficulty urinating or defecating – in combination of numbness or pain down both legs are signs of a central herniation and is a medical emergency. For all other types of disc herniation, a non-surgical approach is effective for up to 90% of patients, with the best conservative treatment being a multi-disciplinary approach.
Vizniak, N. A., Fairweather, L., Murray, N., Hussain, S., DeLapp, D., Eni, G., Davidson, T., & Hedrich, T. (2022). Evidence informed orthopedic conditions. Professional Health Systems Inc.